IR Quarterly
Inside access: Aakash Gupta, MD
By Aakash Gupta, MD
Efficacy of TEPS for patients unsuitable for TIPS
Gupta A, Louie J, Sze D. Transvenous Extrahepatic Portosystemic Shunts (TEPS): Intravascular Ultrasound-Guided Creation of Portocaval, Mesocaval, and Splenorenal Shunts. JVIR, 2026;37.

Tell us about you, your team and your institution.
Aakash Gupta, MD: Our interventional radiology division at Stanford University has a long track record of pioneering new techniques and interventions to improve care for our patients. In fact, the very first report of a percutaneous mesocaval shunt was published in 1996 in the Journal of Vascular and Interventional Radiology by Ulf R.O. Nyman, MD, PhD, and Michael D. Dake, MD, FSIR, using combined percutaneous CT-guided access and fluoroscopy. Current Stanford IR physicians Daniel Sze, MD, PhD, FSIR, and John Louie, MD, FSIR, developed the intravascular ultrasound (IVUS) guided technique for transvenous extrahepatic portosystemic shunt (TEPS) creation.
Why did you pursue this topic?
Dr. Gupta: Endovascular portosystemic shunt creation is a mainstay in the treatment paradigm for complications of portal hypertension, namely variceal bleeding and refractory ascites. However, not all patients are candidates for conventional transjugular intrahepatic portosystemic shunt (TIPS) or even advanced techniques including direct intrahepatic portocaval shunt (DIPS) or portal vein recanalization TIPS (PVR-TIPS). IVUS-guided creation of TEPS is considered a high-risk and last resort option to offer potentially lifesaving portal decompression to pediatric and adult patients, first performed on an exsanguinating child in 2010. Given the rare utilization, prospective randomized data will never be produced, so retrospective evaluation of technical feasibility, patency and long-term adverse events of TEPS is the highest level of evidence that can be generated.
What are the key takeaways from your research?
Dr. Gupta: In a cohort of 24 TEPS creations in 23 patients, IVUS-guided creation of portocaval, mesocaval and splenorenal TEPS was technically successful in all patients with chronic portomesenteric venous occlusion or obstructed intrahepatic path. The 1-year primary patency was 100% and the 3-year primary assisted patency was 100%. Although there were no severe periprocedural adverse events, such as hollow viscus injury or grade 3 intra-abdominal hemorrhage, long-term clinical follow-up identified two rare complications of portopulmonary and hepatopulmonary syndrome. Overall, TEPS is an effective last resort for portomesenteric decompression in patients with obliterated portomesenteric vasculature or an obstructed intrahepatic path.
How might this research influence treatment, practice, or clinical processes in interventional radiology?
Dr. Gupta: TEPS offers another option in the interventionalist’s toolbox for portal decompression, particularly for those experienced with side-firing IVUS. Patients with chronic portomesenteric venous occlusion or obstructed intrahepatic path and who are not candidates for TIPS, DIPS or PVR-TIPS may benefit.
What were the key technical decision points that determined whether a portocaval versus mesocaval or splenorenal shunt was created in individual patients?
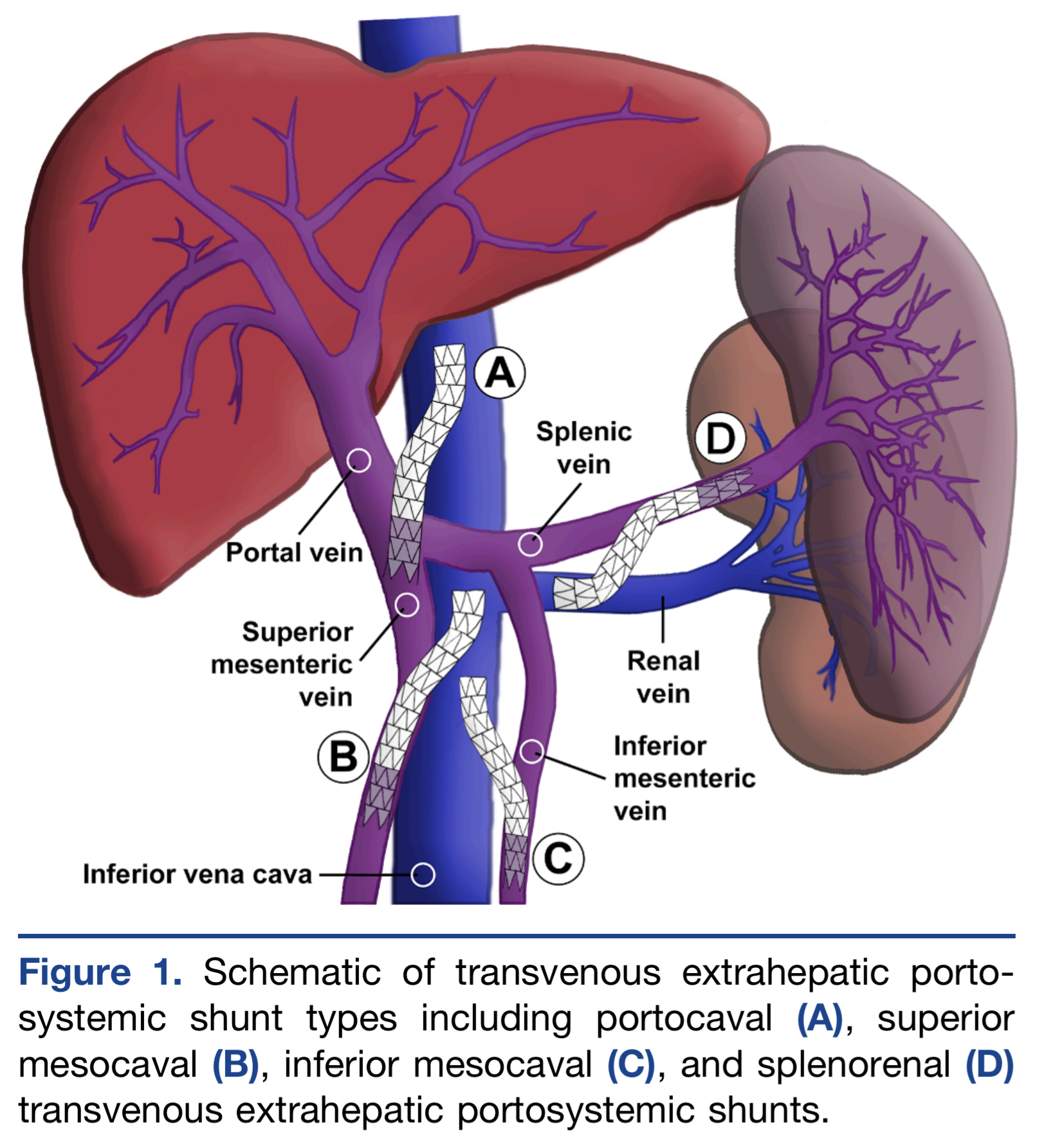
Dr. Gupta: The study includes a heterogenous group of TEPS, including portocaval, superior and inferior mesocaval, and splenorenal shunts. Each patient had unique portomesenteric venous anatomical deformity, requiring meticulous review of pre- and intraprocedural imaging to design a safe pathway between systemic and portomesenteric veins.
Given the 100% patency outcomes, what factors do you think contributed most to long-term durability in this cohort?
Dr. Gupta: Several different techniques have been described for creation of TEPS, including transabdominal through-and-through puncture of the superior mesenteric vein into the inferior vena cava and transmesenteric puncture of the inferior vena cava via mini-laparotomy. However, the IVUS- guided technique presented in our study has benefits of superior intraprocedural visualization of intervening structures as well as a single wall puncture into the target vein. This may minimize vessel trauma and intestinal flora contamination. Also, since the TEPS path is extrahepatic, there is no communication with the biliary system, and the path lengths tend to be short.
How should clinicians weigh the risk of post-procedural hepatic encephalopathy when considering TEPS in patients who are not TIPS candidates?
Dr. Gupta: New or worsened hepatic encephalopathy is a risk with all portal decompression techniques, and the rate in our cohort was equivalent to that reported with TIPS. Standard informed consent, shunt dimension optimization, collaboration with hepatologists, and prophylactic and therapeutic medications apply to TEPS. No patients required shunt reduction or occlusion.
Any next steps or plans for follow‑up research?
Dr. Gupta: We are starting to favor techniques to decompress portal and splanchnic venous hypertension that may preserve or even increase trophic hepatopetal flow. Also, forward-firing IVUS may become available and may further broaden the potential for navigation and creation of unconventional shunts.